Aortic arch repair is indicated for aneurysmal disease of the aortic arch (degeneration or chronic dissections) in asymptomatic patients when the size of the aortic arch exceeds 5.5 cm. In patients with acute aortic dissection, it is reasonable to repair the entire aortic arch when the arch is aneurysmal, or there is extensive aortic arch destruction and leakage.
Repair is also indicated when there is an infected (mycotic) aneurysm or when there is significant atherosclerosis (plaque) in the arch that has resulted in strokes. Also, a growth rate of more than 0.5 cm/year in the absence of symptoms could be considered an indication for operation.
Symptoms associated with aortic arch aneurysms such as hoarseness, difficulty in swallowing, difficulty in breathing, and chest or back pain are indications for operative intervention.
Arch open repair
For patients with isolated aortic arch aneurysms less than 4.0 cm in diameter, it is reasonable to reimage using computed tomographic imaging (CT scan) or cardiac magnetic resonance imaging (Cardiac MRI), at 12-month intervals, to detect enlargement of the aneurysm.
For patients with isolated aortic arch aneurysms 4.0 cm or greater in diameter, it is reasonable to reimage using computed tomographic imaging or cardiac magnetic resonance imaging (Cardiac MRI), at six-month intervals, to detect enlargement of the aneurysm.
Aortic arch procedures require temporary interruption of the blood flow to the blood vessels that supply the brain. For safe interruption of the blood flow to the brain the core temperature of the body needs to be progressively reduced to 18 to 20 degrees Celsius (deep hypothermia). In that cold body temperature, the metabolism is reduced significantly, and it allows cessation of the blood flow to the body for 30 to 40 minutes without side effects.
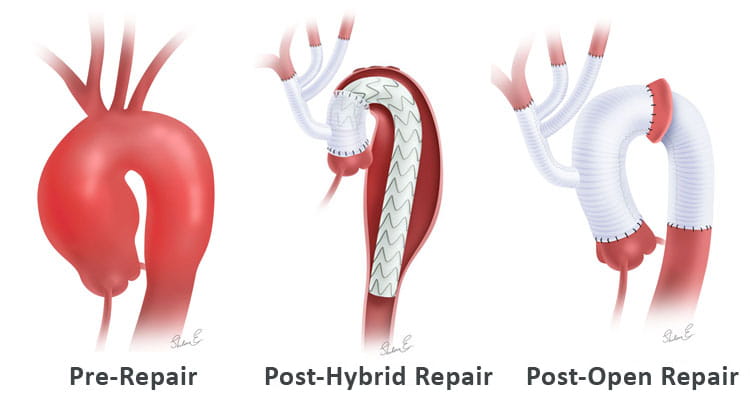
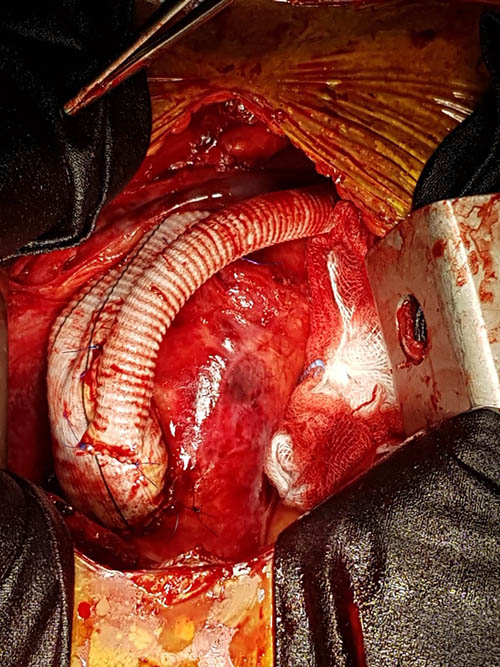
Under these conditions, the aortic arch is replaced with a synthetic tube which is attached to normal segments of the ascending and descending thoracic aorta. The arch blood vessels (brachiocephalic, left carotid, and left subclavian arteries) that supply the brain amongst other organs are reconnected to the synthetic graft with a separate synthetic tube with three branches (trifurcation graft). While all these connections are being created, this novel technique allows for insertion of catheters in the individual arch blood vessels for perfusion of the brain with blood (selective cerebral perfusion).
In certain circumstances one can replace only the undersurface of the aortic arch, leaving intact a narrow strip of the upper part of the aortic arch containing the arch vessels (hemiarch technique). This simplified method requires invariably a shorter period of hypothermia and reduces significantly the complexity of the operation.
Aortic arch and descending thoracic aortic repair
Aneurysms of the aortic arch are commonly associated with aneurysms of the ascending aorta or the adjacent descending thoracic aorta. The indications for operative intervention in these patients are those for the largest aortic aneurysm.
An operation in this area is done in two stages:
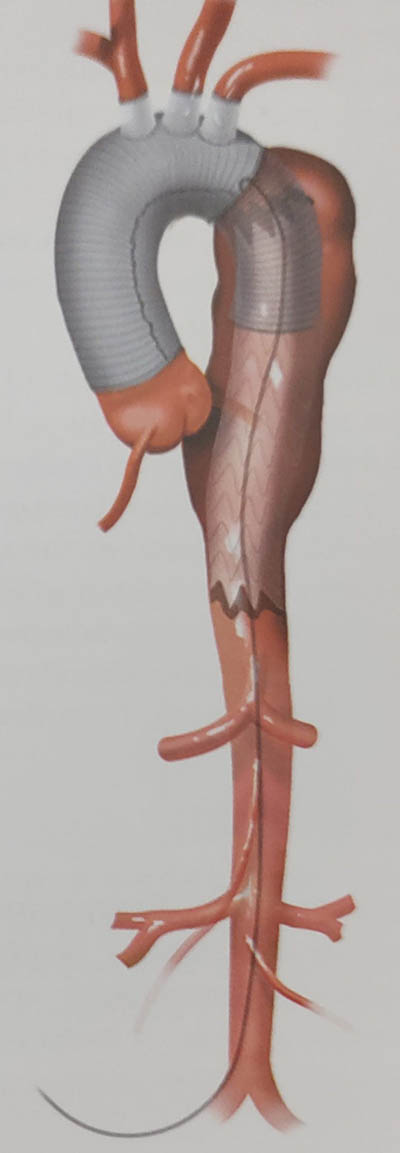
- Stage I – In the first stage the ascending aorta and aortic arch is replaced using the elephant trunk technique.
- Stage II – An "elephant trunk" procedure is used to provide a Dacron graft landing zone for open or endovascular stent graft treatment of the descending thoracic aortic aneurysm.
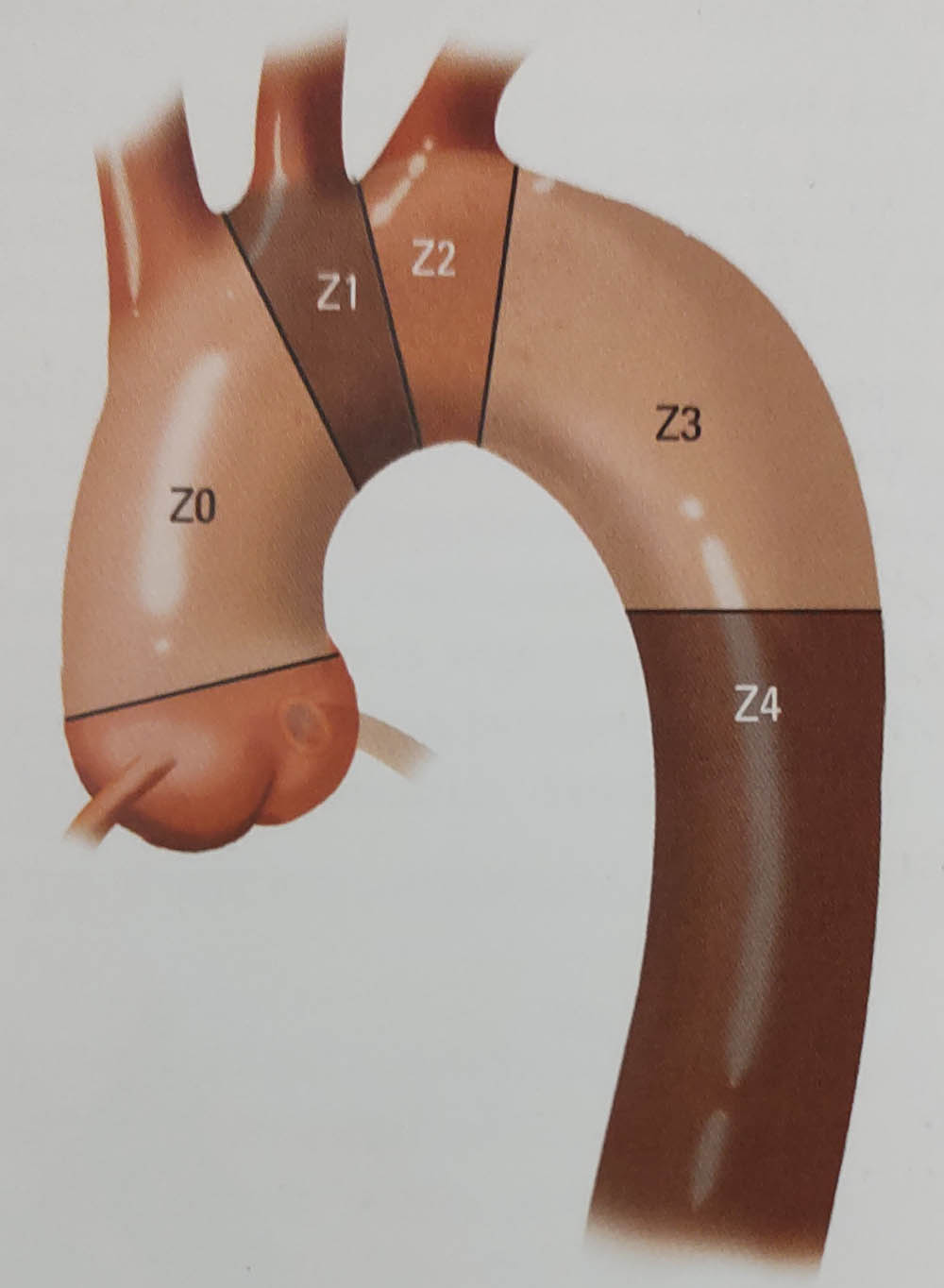
Classification of landing zones for TEVAR. Zone O includes the ascending aorta up to the innominate artery. Zone 1 includes the aorta from the innominate artery to the left carotid artery. Zone 2 includes the aorta from the left carotid to the left subclavian artery. Zone 3 includes the proximal descending aorta distal to the left subclavian artery and Zone 4 includes the mid descending aorta.
Type 1 hybrid repair of the aortic arch. The arch vessels are sequentially revascularized following the proximal surgical anastomosis.
This is followed by deployment of a stent-graft either in an antegrade or retrograde technique.
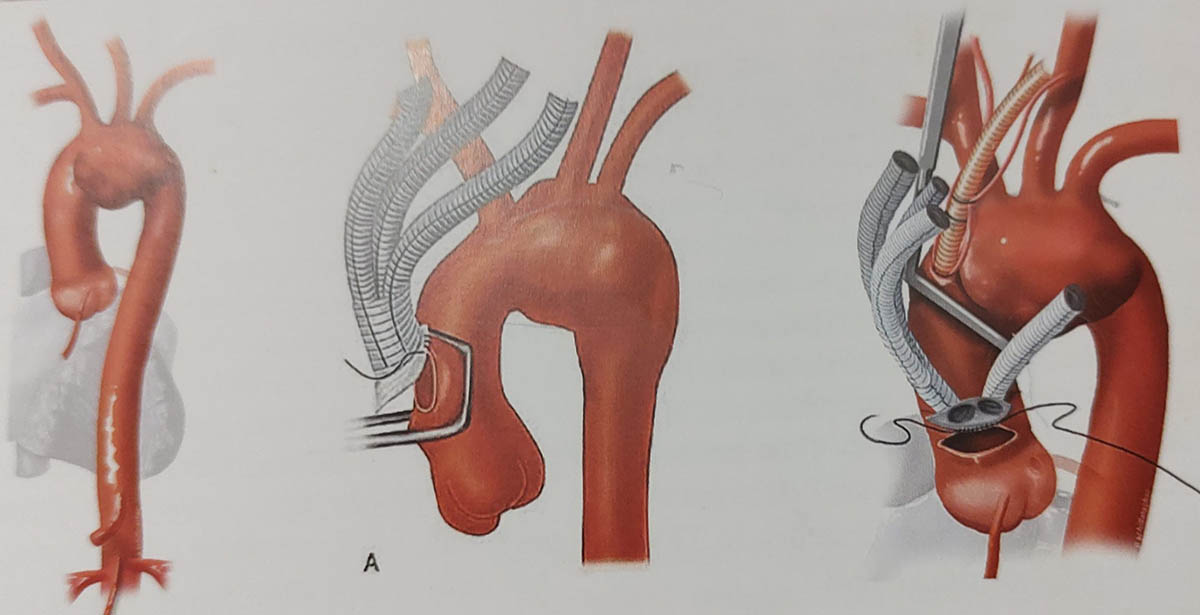
Aortic arch debranching for hybrid repair – grafts from ascending aorta to Right Brachiocephalic Rrtery, Left Common Carotid Artery and Left Subclavian Artery to facilitate Zone 1 Endovascular repair.
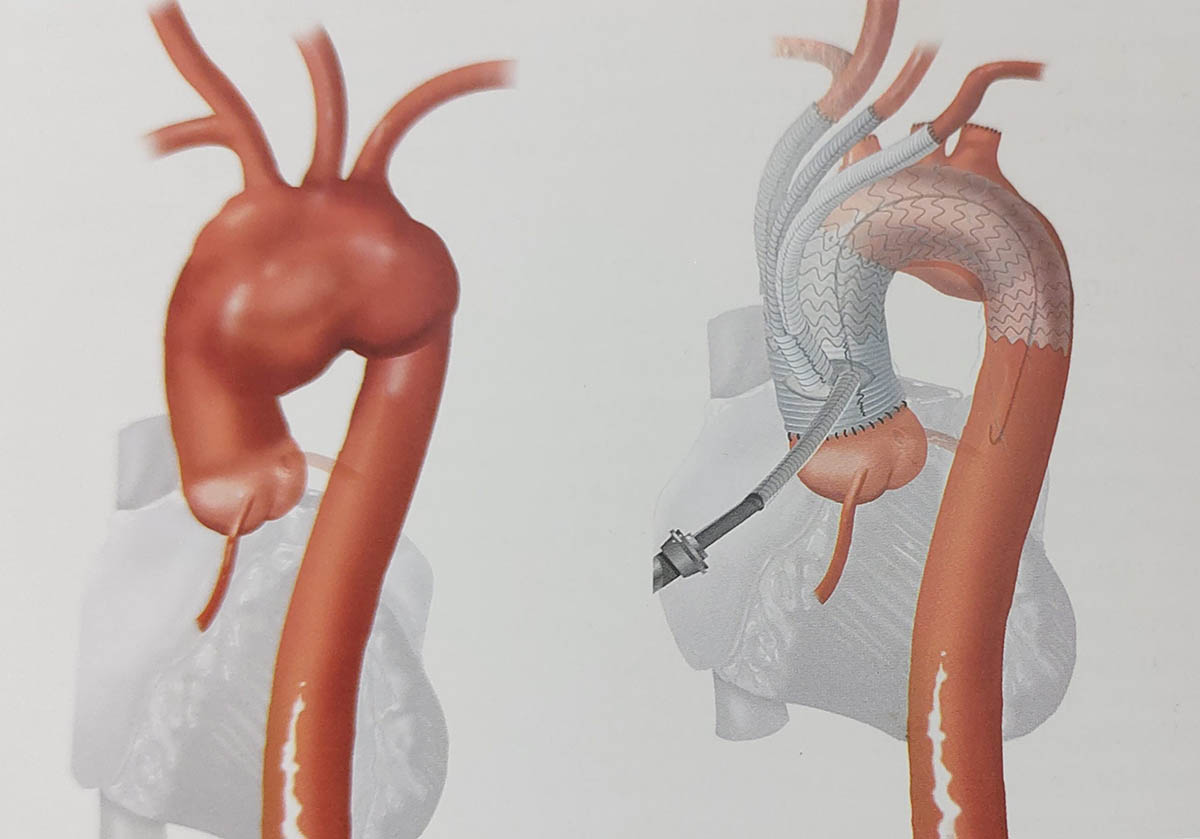
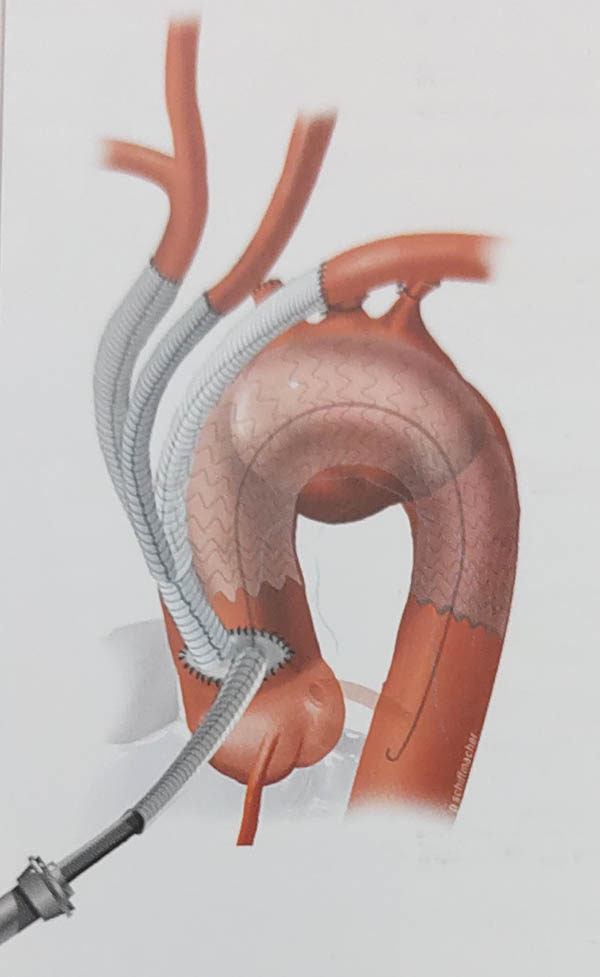
Type 2 repair where the arch vessels are revascularized along with the replacement of the ascending aorta to create a landing zone 0 for the TEVAR. This figure demonstrated antegrade deployment of TEVAR.
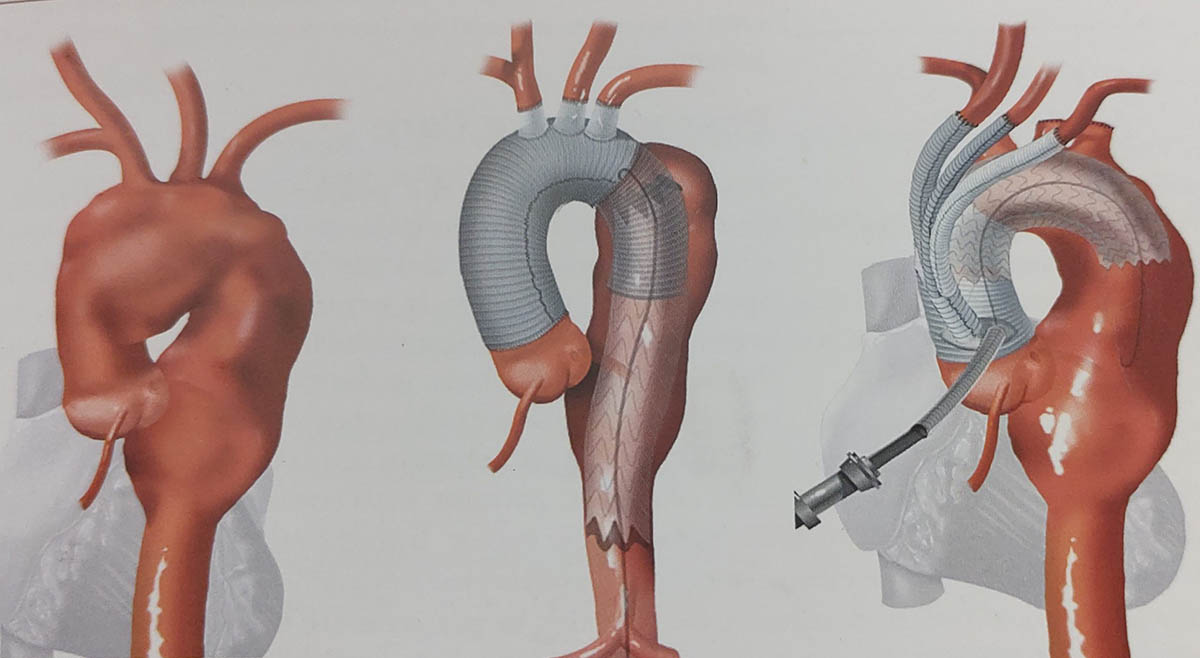
Type 3 repair where the first stage includes replacement of the ascending aorta and arch vessels with an open or stented elephant trunk.
The second stage includes a TEVAR to exclude the distal thoracic aortic aneurysm.