Aortic root disease is often asymptomatic and diagnosed during imaging. To avoid acute aortic syndromes and dissections in aortic root aneurysms (and/or ascending aorta aneurysms), prophylactic surgery of the aortic root should be performed when indicated according to the recommendation of the American Heart Association and European Society of Cardiology guidelines: irrespective of the presence and severity of an associated aortic valve regurgitation, surgery is indicated in patients who have aortic root disease with maximal ascending aortic diameter > 50 mm, even before in case of cardio-vascular risk factors.
Bentall Procedure
Replacement of the aorta and of the aortic valve using a composite-graft replacement with an aortic valve prosthesis has been the standard for decades. This technique is well known as “Bentall procedure” which means implantation of a mechanical-valve conduit and the concomitant requirement for long-term anticoagulation.
Coronary arteries are localized at the surface of the heart, that makes their access easy.

This procedure can also be done using a bio-prosthesis (Bio Bentall Procedure). This avoids need for anticoagulation therapy but are more prone to structural valve deterioration over time.
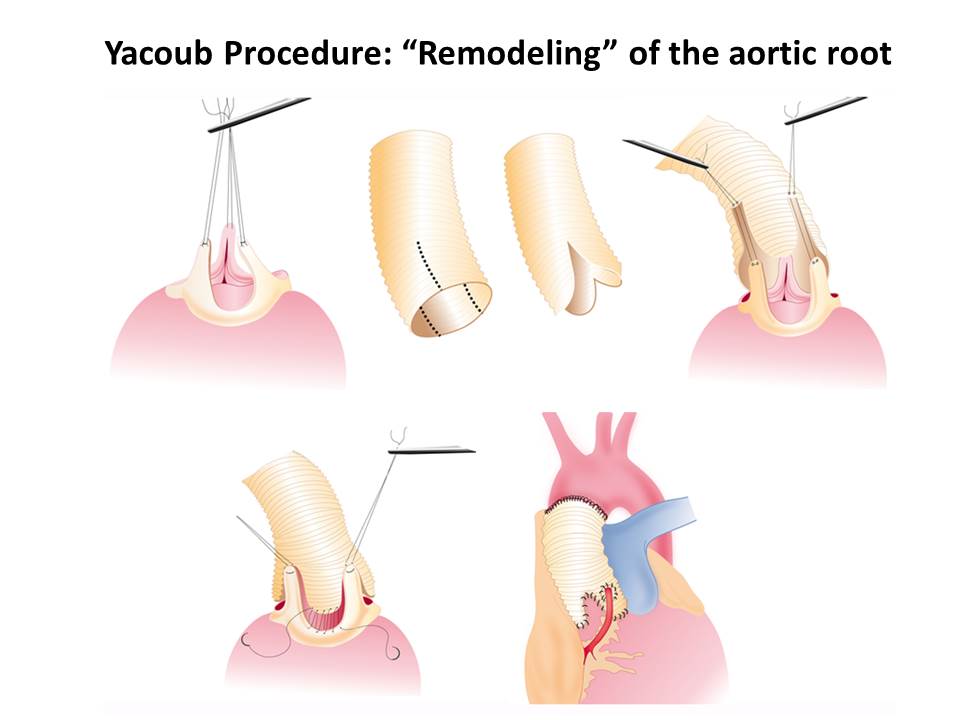
Valve-sparing
Valve-sparing aortic root replacement has become a well-established option for patients with aortic root aneurysms who have morphologically normal tricuspid or non-calcified, pliable bicuspid aortic valves. Valve-sparing aortic root replacement operations are subdivided into 2 general families: (1) the Yacoub “remodeling” technique used since 1979 and (2) the David “reimplantation” technique performed since 1988.
The remodeling technique provides physiologic cusp movement within the 3 reconstructed neo-sinuses, thus preserving root expansibility through the interleaflet triangles, but it does not address annular base dilation. Root remodeling continues to be a viable option in valve-preserving root replacement. If combined with careful assessment and, if necessary, correction of aortic valve form, reproducible restoration of aortic valve function can be achieved. The concept of root remodeling also can be applied to bicuspid or unicuspid aortic valves, although long-term durability is inferior with nontricuspid anatomy of the aortic valve. Because of the lack of annular stabilization, it must be reserved in non-dilated aortic annulus.
The reimplantation procedure as an inclusion technique performs a subvalvular annuloplasty through the proximal suture of the graft but withdraws the sinuses of Valsalva and includes the interleaflet triangles within the noncompliant prosthesis, thus impairing root dynamics. Furthermore, most failures of reimplantation procedures are due to cusp prolapse, either residual or induced by root reconstruction, and re-suspension of the cusp effective height is more and more mandatory.
David Procedure
